
Tradeoffs of Surgery vs. Chemo for Testicular Cancer
Tradeoffs of RPLND surgery vs. BEP Chemotherapy for Stage 2 Testicular Cancer Patients

Tl;dr - Stage 2 Testicular Cancer patients may have a choice between chemotherapy and a surgical procedure called an RPLND. These patients should seek out surgeons at a high volume center for RPLND to help them compare / contrast the risks of both treatments. RPLND could be a meaningfully better treatment option for these patients.
1 in every 270 males will be diagnosed with testicular cancer at some point in their lifetime. The majority of those affected are young adults between 20 to 35 years of age. In fact, testis cancer (TC) is actually the most common type of malignancy among men in that age range, and thus, is often these young adults’ first personal brush with Cancer.
That was certainly (and luckily) the case for me. I was diagnosed with Stage 2B TC in 2024 at the age of 28. I knew relatively little about cancer(s) and cancer treatments, so the 30 days after diagnosis were a mad dash to come up to speed on different terminologies, risk factors, treatments, etc.
Fortunately for us modern day TC patients, a doctor named Lawrence Einhorn at Indiana University developed a platinum-based chemotherapy regimen based on three chemicals: Bleomycin, Etoposide, and cisPlatin (BEP). The combination of drugs is incredibly effective at fighting TC’s germ cell tumors. After the development & refinement of BEP chemo, TC now has a 5 year survival rate of 95%.
Given the success rate of BEP chemo, you will likely find that oncologists and urologists are quick to strongly recommend it for any Stage 2 or Stage 3 TC patient that has had cancer migrate to other areas of their body (TC has no stage 4). For stage 3 patients, this is likely the only (and best) option. But for Stage 2 patients like myself, you may have the ability to choose between two treatment options:
Chemotherapy - 3 round of BEP (bleomycin, etoposide, cisplatin), a platinum based chemotherapy
Retroperitoneal Lymph Node Dissection (RPLND)- a surgical procedure where a surgical urologist removes the lymph nodes from your abdomen
Your doctor will likely point you to this document, where the National Comprehensive Care Network documents the standards of care for every stage & type of TC. Here, you’ll find pages like this, that indicate those two options I described:
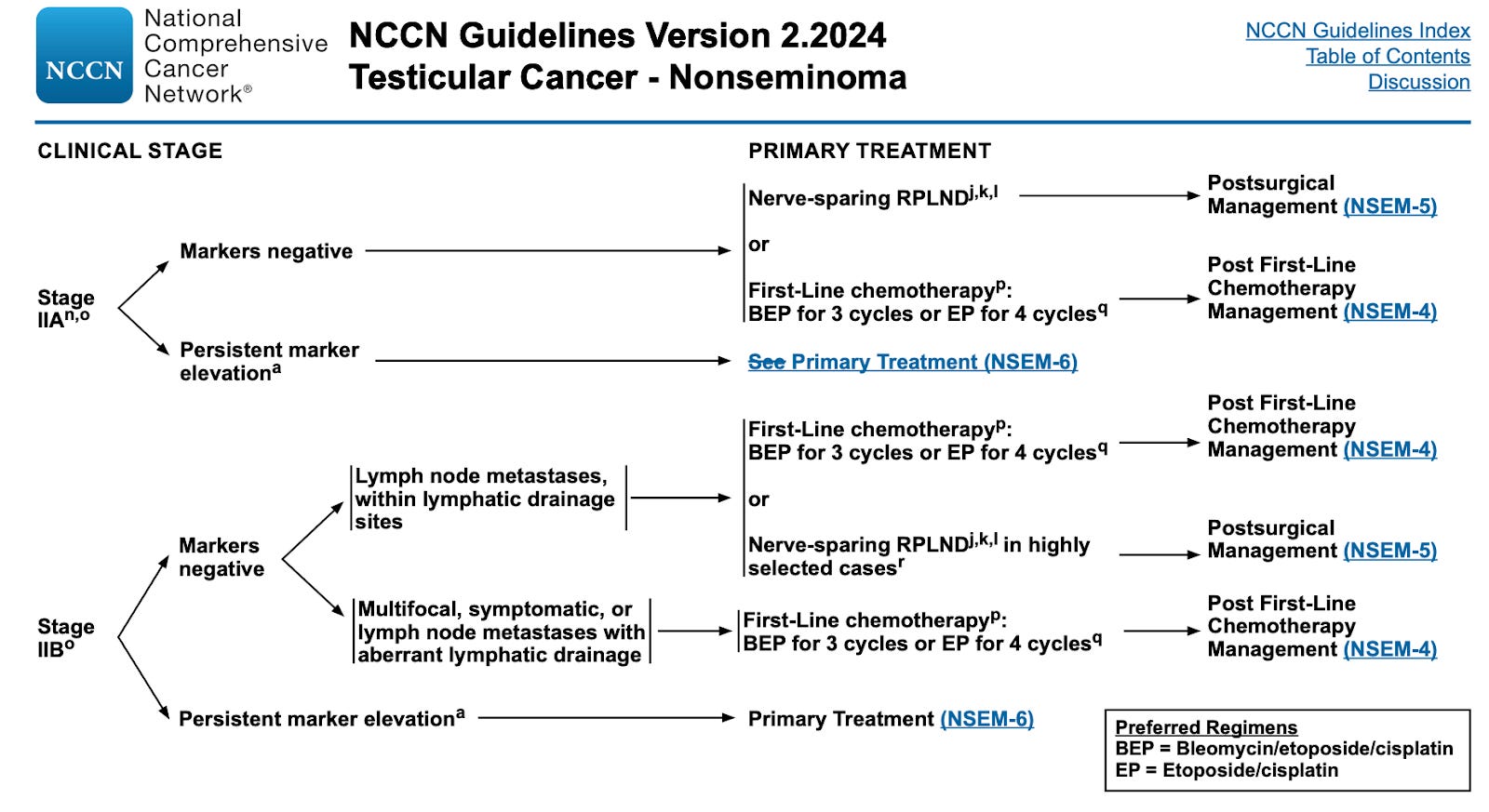
Above is depicted the recommended care options for Stage 2A or 2B patients with nonseminoma.
RPLND has also been around for 70+ years, but in the last 20 years, has gained more traction. Whether RPLND or chemotherapy are best for your specific medical situation should be consulted with (ideally multiple) doctors. However, I’d like to encourage any Stage 2 patient to explore RPLND as an option with your doctors. My experience was that many oncologists and urologists were heavily biased against RPLND, some even describing it as “a barbaric procedure that is not commonly conducted anymore”. RPLND is a highly specialized procedure, and most urologists do not perform them with any regularity.
Admittedly, RPLND is a scary surgical procedure, but it has some serious advantages over chemo, and some of the latest science from high volume RPLND centers is quite compelling.
The science on Primary RPLND as a compelling cure for Stage 2 TS cancer
Testicular cancer comes in 3 stages (in increasing order of severity). While the actual details of staging are complex (see TNM staging here if interested), it roughly breaks down to:
Stage 1 (local): Cancer has not yet migrated to other parts of the body.
Stage 2 (regional): Cancer has spread to nearby structures or lymph nodes, usually the abdomen
Stage 3 (distant): Cancer has spread to distant lymph nodes or structures, often the brain or lungs
Primary RPLND is most commonly performed for Stage 2A or 2B patients that have had cancer spread to their retroperitoneal area (the most common “next stop” for TC) but are still tumor marker negative.
In fact, recent studies in the last 5 years are starting to prove that RPLND has a high chance of being curative in these Stage 2 patients, for both seminoma and nonseminoma tumors:
For seminoma tumors: A joint study across US health institutions (SEMS Trial) found that RPLND in Stage 2A and 2B seminoma patients had a 2-year recurrence free survival rate of 81%, with only 7% of patients experiencing some kind of short- or long-term complications (source). A similar study at MSK also found a 81% 2-year survival rate for stage 2A/2B seminoma patients that received primary RPLND (source) Another European study here (source)
For nonseminoma tumors: A study at IU Health in 2022 found that RPLND had a 80% 2-year recurrence-free survival (RFS) rate, and a 79% 5 year RFS, even in the presence of more aggressive subtypes like embryonal carcinoma (source). Similarly, another German study back in 2000 recommended RPLND in an effort to spare patients (source).
The successes of RPLND in these papers suggest that chemotherapy (both primary and adjuvant) could be over-treating many stage 2 patients.
Of course, there is a glaring detail in what I just shared. The proposed remission-free survival rates are only around 80% for primary RPLND, which is lower than primary chemotherapy’s 95-98% RFS rate. Nothing to fear though, the 20% of patients that do recur after primary RPLND, will be able to pursue adjuvant chemotherapy (likely 2-3x BEP) and have the same survival rates. Not an ideal path to remission for those 20%, but an effective one.
Pros & Cons of RPLND
Primary RPLNDs main advantage is attempting to avoid the toxicity of chemotherapy, and thus, avoiding the short- and long-term health risks associated with chemo. The short- and long- term risks / effects, along with the pain & recovery risks of RPLND are comparably much better than chemo (see below):
Short term risks/effects: Short-term risks of RPLND are mainly those associated with that of any complex surgery. These can be largely mitigated at any high volume surgery center. Compare that to chemotherapy, whose short term effects include neuropathy (from the etoposide), lung damage (from the bleomycin), and tinnitus in the ears (from the cisplatin)
Long-term risks/effects: The long-term risks of RPLND are a 5-10% chance of retrograde ejaculation, a 1% chance of hernia, and a 6-12 inch scar on your abdomen. Compare those to the long term risks of an aggressive chemotherapy like BEP, which include a 1-2% increased risk of other cancers, 1-2% increased chance of cardiovascular disease, 30% chance of infertility
Duration & experience: The RPLND procedure is usually 3-5 hours long followed by a 3-5 day hospital stay. The subsequent recovery is 6-8 weeks long, with the first three weeks being the hardest. A standard course of 3xBEP chemotherapy is long - it’s three, 3 week cycles of BEP chemical infusions for a total of 9 weeks (2 months) minimum. The first week of each 3 week cycle is 8+ hour long days in the hospital hooked up to IVs. Couple those 9 weeks of infusions with another 2-3 months of recovery time to get back to “normal”.
Discomfort: Personally, I found that week 1 after the RPLND was massively uncomfortable and painful. Week 2 was massively uncomfortable still but the pain was limited. By week 3, I was only uncomfortable when walking or in certain awkward positions. Week 4 onward I had a near-full range of motion, but medical restrictions dictate I not lift anything heavier than 10 pounds until week 7.
The major trade off for these advantages though (as indicated in the scientific articles listed above), is that RPLND only has an 80% chance of being curative, and that percentage can vary based on certain risk factors. In fact, I had different urologists and oncologists quote me numbers in the range of 60-85%. Exact percentages depend on a whole host of medical information (blood markers, tumor type & sub type, # and size of lymph nodes, other characteristics like LVI, etc.).
I’d encourage TS patients that are considering RPLND to think about what that really means for you. You will spend the next 5 years with a meaningful chance (15% or more) of still having cancer. I often see cancer patients who have completed chemotherapy and declared themselves in remission post videos of them ringing bells while nursing staff, family, and doctors clap for them, having successfully beaten cancer. As someone who opted for RPLND, I will never get to do that. I’ll just cross my fingers everyday for the next 1,825 days. For some, this may be too daunting of a mental hurdle to wake up to everyday. For others, this may be acceptable risk.
I have Stage 2 testicular cancer, what should my next steps be?
It’s crucial to note that RPLND may not be the right treatment option for you. I am merely highlighting the advantages so that you aren’t dissuaded from evaluating it entirely if your local oncologist shrugs off the procedure.
A few things that were particularly helpful for me.
Speak with a doctor that does a high volume of RPLND procedures. RPLND is a highly specialized procedure, and most urologists do not perform them with any regularity. An RPLND performed at a high volume center by a surgeon that specializes in them increases the likelihood of the procedure being curative, and decreases the risks of short- and long- term side effects. Indiana University Health and Memorial Sloan Kettering in the US are the two best centers for TC and RPLND specifically. Both have the infrastructure setup to provide consulting opinions on your TC case.
Find a doctor that you trust to take the lead on your case. Cancer stays with you for life. Even after remission, you will likely remain at higher risk for cancers for the remainder of your life, requiring testing every year. While seeking out multiple medical opinions is crucial, it’s just as critical to settle on a doctor that you trust to lead you through your treatment and can be your primary thought partner as you tackle the new day-to-day challenges that come up.
Be Optimistic. The 5yr survival rate for TC is 95%+. We can thank Dr. Lawrence Einhorn at Indiana University and patient John Cleland, who bravely pioneered a platinum based chemotherapy that is now the incredibly effective BEP chemotherapy. And we can thank urologists like Tim Masterson at IU who have refined & mastered alternative surgical procedures like RPLND.
If you’ve been diagnosed with TC and need someone to talk to, please reach out. I’d be happy to talk.
And lastly, a big thank you to Dr. Masterson who performed my successful RPLND, and to Dr. Einhorn who consulted heavily on my case.